
A doula’s guide to Induction: Part 1

This is Part I in a 3 part series on Induction, where I discuss what induction is and how to decide if it’s right for you.
In Part II, we’ll talk about how they are done, and what to expect and plan for when you’re heading in for an induction. Then, in Part III, I share lots of tips and tricks for a positive, autonomous induction experience.
As a doula, I see the topic of induction come up a lot. During the pandemic, it has become even more prevalent.
You may be here because your doctor has suggested induction as a good option for you, or you may have been told that you need one. Or, you may just be doing your homework in case it comes up later.
Wherever you are in your birthing journey, it is really important to know the ins and outs of induction so that you can decide if it is the right choice for you. The worst thing to do is to head into an induction without doing your research.
WHAT IS INDUCTION?
Induction - or to induce - means to artificially start the labor process. There are both non-medical and medical methods of induction.
WHY INDUCE?
There are many reasons given for wanting to do an induction – not all of them evidence-based. These are the most common reasons for having an induction:
◇ Medical indication in the mother (gestational diabetes, preeclampsia, cholestasis)
◇ Medical indication in the baby (problem with restricted growth, fetal distress, placental deterioration)
◇ Suspected “big” baby (note this is not medically indicated - and not evidence-based.)
◇ Baby is post-dates (after 41-42 weeks, depending on your provider’s policy)
◇ Mother’s preference – tiredness, support person availability, etc
◇ Caregiver’s preference – baby past 40 weeks, availability, etc.
Has your care provider quoted the ARRIVE study as the reason you should induce - or said something along the lines of “Studies show it’s safest to induce labor at 39 weeks”? Read this first.
DOES IT WORK?
For an induction to be successful, several factors come into play. Remember the 6 processes that need to happen for labor to progress? They are also indicators for whether an induction will work. The amount of dilation and effacement of the cervix, along with the station (where the baby’s head sits in relation to the pelvis), and the cervical position and ripeness, determine how likely it is for an induction to be successful in kick-starting your labor. In plain terms, the cervix needs to be soft and thin in order for it to open, and baby needs to descend to start your body contracting efficiently. If your cervix isn’t ready, it’s likely that induction will take a long time or need added interventions. In a medically indicated induction, it’s likely your body won’t be “ready”; there are many ways to start the cervix off on its journey to opening, and most of the time they do work, though it takes time and stamina.
BISHOP SCORE
Have you heard of the Bishop Score? It is a system of “scoring” to tell us the likelihood of the body being responsive to being induced. Here’s how it works: the higher the score, the more likely induction will work smoothly and quickly, or that your body will labor without needing extra help. A score of 8 or higher is means the body is ready for labor and favorable for induction (or, it could be argued, favorable for waiting until it happens spontaneously). Scores lower than 5 are called “unfavorable” - suggesting that induction will not work as smoothly.
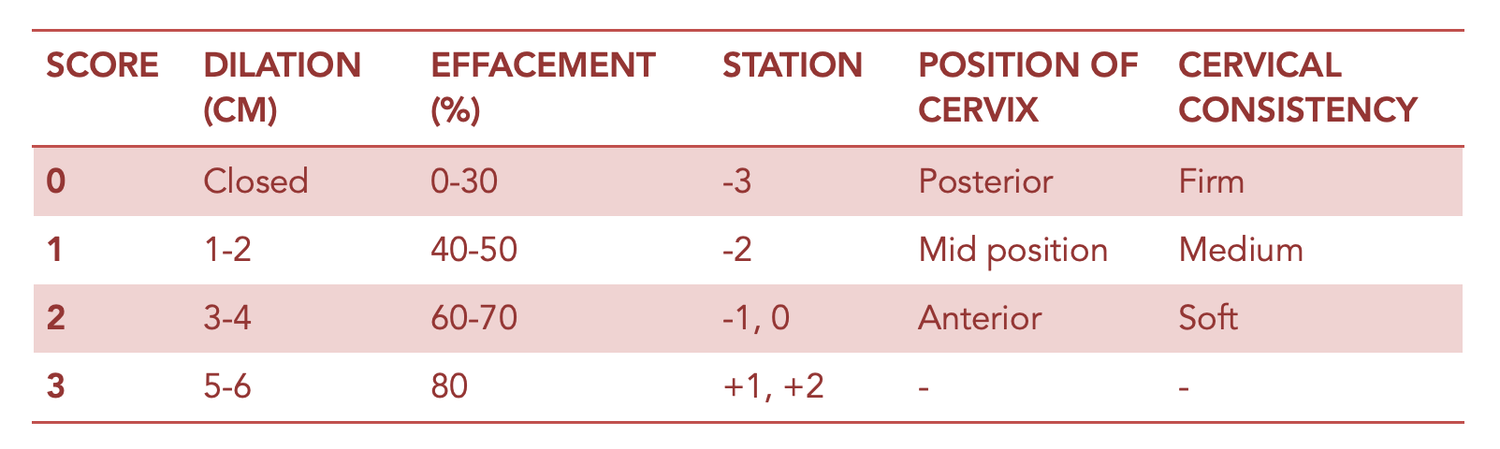
CHART FOR DETERMINING THE BISHOP SCORE
BE INFORMED
Not all care providers will discuss the Bishop Score with you! Please know that you have a right to ask, or to question any decision or possible procedure during your pregnancy and birth – it’s a good idea to know the readiness of your body before deciding to go ahead with an induction, so you have an idea of what to expect.
SO SHOULD I INDUCE OR NOT?
Only you can make the decision, but as long as you’re informed about all your options and know what an induction involves, there is no wrong answer. If you’re getting pressure to induce from your care provider and there’s no medical indication, an easy answer would be not until your body and baby are ready. It can be very hard, especially as your due date approaches (and perhaps passes), to be patient - especially if you have no signs that your labor is near. Finding your late pregnancy zen - patience, acceptance and calm - can help. So can doing your research about what induction entails, so you can make an informed decision. If you’re really feeling stressed, it can help some people to book the date in, knowing that it’s on the calendar - and then you can always cancel if you’re not feeling ready on the day. Sometimes just the action of deciding to do it helps alleviate the worry and labor starts off on its own. A bit of reverse psychology, birth style!
If there is an evidence-based medical indication - if something is wrong with you or your baby - then yes, induction may be the right answer, and one you don’t have much choice over. In that case, preparing for an autonomous, positive induction process helps a lot! And I’ll cover more on that in the final part of this series.
Part II (The Induction Process explained)
Part III (Tips and Tricks for a great Induction experience)
Please note! I’m not a doctor. I’m not here to offer medical advice. The information in this post is to help you build a well-rounded knowledge of inductions so you can make the right decision, along with the advice and guidance of your doctor or midwife.
Illustration by Mercedes DeBellard - here’s her instagram and her website